 By Terri Leonard
By Terri Leonard
Editor’s note: The following is an email sent to the WAC by Dr. Leonard regarding an issue that came up at last month’s WAC meeting regarding the fluoridation issue
Dear Members of the Water Advisory Committee,
I am sending this email to present evidence to refute Dr. Lyman’s statement during the April 25, 2013, Water Advisory Committee meeting that declining dental caries rates in European countries that do not fluoridate their water supply can be attributed to fluoride added to the salt and milk supply in those countries.
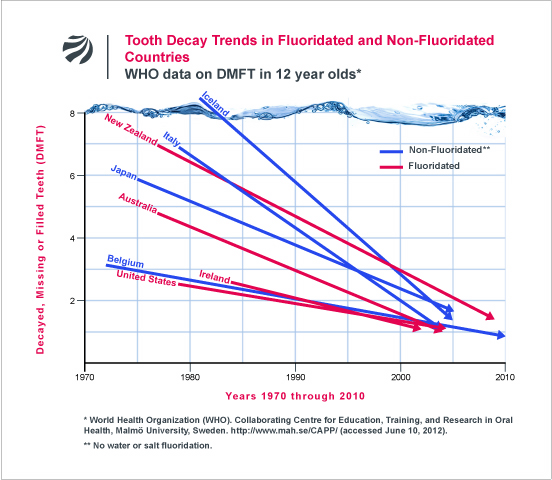
WAC member Mark Siegler asked the pro-fluoridation presenters at the last WAC meeting to comment on the series of graphs that show that over time the number of caries among children is falling, irrespective of the fluoride content of their drinking water. Dr. Donald Lyman responded that other countries add fluoride to salt or milk. He stated that “These data [the graphs] are provided through the World Health Organization, and it shows a uniform decline, as you say, with dental caries, both in the young and in the old, with the application of fluoride. It’s applied in different ways in different countries. In some countries in Europe, they use it in the salt supply, in some countries they put it in the milk. So they’re different modalities, and they provide a different kind of outcome at the other end because of those who consume whatever the product is.”
Mark Siegler asked later on for clarification regarding whether it is the position of the pro-fluoridation presenters that the low caries rate in populations that are not drinking fluoridated water is due to the consumption by those populations of other fluoridated products, such as milk. Dr. Lyman affirmed that this is the case, and he stated, “The application of fluoride in some methodology, in most of Europe is fairly uniform.” Dr. Lyman then reaffirmed that salt, water, and milk are the modalities in Europe used to deliver fluoride. Mark Siegler then asked for “the breakdown across countries as to who does what.” Dr. Lyman responded, “I have a list I can show you.” I am not aware if Dr. Lyman ever provided such a list to WAC members at some point after the April 25 meeting. However, I have data that I would like to provide.
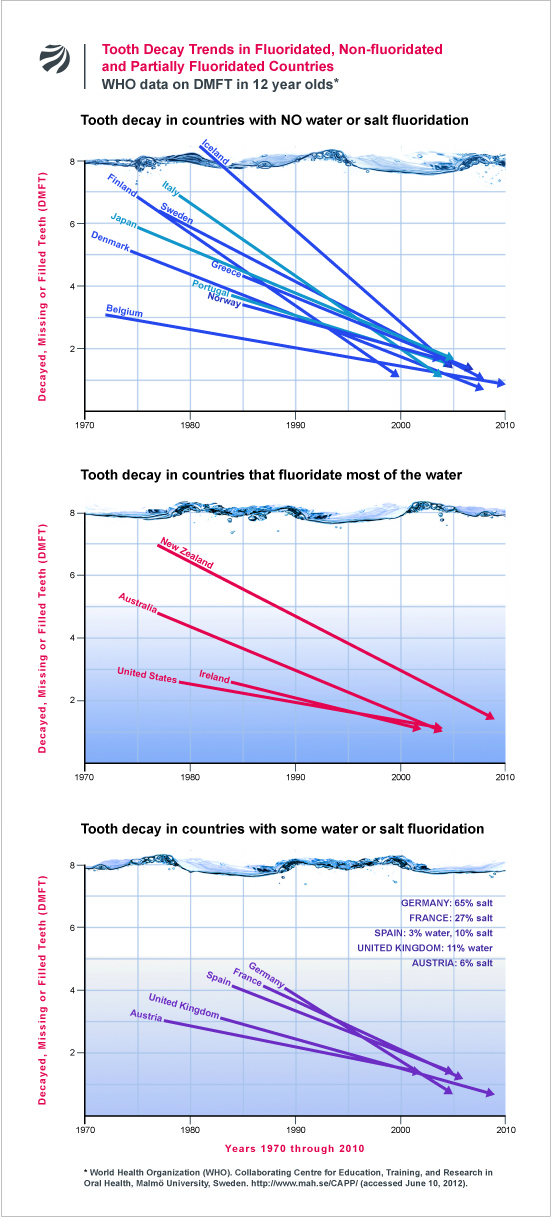
I am including, below, graphs and a table that contradict Dr. Lyman’s assertion that the declining dental caries rates in countries that do not fluoridate their water supply can be attributed to fluoridation of the salt or milk supply of those countries. These data indicate that there are many countries that do not supply fluoride in either their water or salt, and yet these countries are experiencing the same decrease in tooth decay as countries that either fluoridate most of their water or fluoridate some of their water or salt. These graphs and table can be found at http://www.fluoridealert.org/studies/caries01/ . Please visit this link to see much more additional information on this topic, including published research and commentary on the decline in tooth decay in the western world, and, below that, information about tooth decay trends in specific European countries.
Note that the graphs and table below address the issue of water and salt fluoridation. Milk fluoridation is not practiced in any of the countries included in the graphs and table except for the UK; therefore, milk fluoridation is not the cause of the low dental caries rates indicated in the graphs and table for countries that do not add fluoride to their water or salt.
If the following graphs and table are not visible (which can happen with certain email filters), please view them here http://www.fluoridealert.org/studies/caries01/
|
DMFT (Decayed, Missing & Filled teeth) Status for 12 year olds by Country |
|||
|
Country |
DMFTs |
Year |
Status* |
|
Denmark |
0.7 |
2008 |
No water fluoridation. |
|
Germany |
0.7 |
2005 |
No water fluoridation. |
|
England |
0.7 |
2009 |
11% water fluoridation. |
|
Netherlands* |
0.8 |
2002 |
No water fluoridation. |
|
Switzerland** |
0.82 |
2009 |
No water fluoridation. |
|
Belgium |
0.9 |
2009-10 |
No water fluoridation. |
|
Sweden |
0.9 |
2008 |
No water fluoridation. |
|
Australia |
1.0 |
2003-2004 |
80% water fluoridation. |
|
Austria |
1.0 |
2002 |
No water fluoridation. 6% salt fluoridation. |
|
Ireland |
1.1 |
2002 |
100% water fluoridation in study. |
|
Italy |
1.1 |
2004 |
No water fluoridation. |
|
United States |
1.19 |
1999-2004 |
64% water fluoridation. |
|
Finland |
1.2 |
2006 |
No water fluoridation. |
|
France |
1.2 |
2006 |
No water fluoridation. |
|
Spain |
1.3 |
2004 |
11% water fluoridation. |
|
Greece |
1.35 |
2005-06 |
No water fluoridation. |
|
Iceland |
1.4 |
2005 |
No water fluoridation. |
|
New Zealand |
1.4 |
2009 |
61% water fluoridation. |
|
Japan |
1.7 |
2005 |
No water fluoridation. |
|
Norway |
1.7 |
2004 |
No water fluoridation. |
|
* The Hague | ** Zurich |
|||
|
Tooth Decay data from:
Salt fluoridation data from:
|
|||



The graphs put forward by Dr. Leonard are not in dispute and certainly show a decrease in cavities across many populations. However, they do not refute the point made by Dr. Lyman, nor do they tell the whole story about the various reasons for the drops in dental caries across countries.
The point Dr. Lyman was making was a specific one that some countries have chosen ingestion of fluoride in mild or salt as an alternative to water, not that this was the only alternative. Topical application is another effective option, but implies ready and affordable access to a dentist who can apply fluoride topically, and or a pediatrician who can prescribe drops.
Such ready access is available in countries such as Iceland ( note the very steep slope of the decline ) which has no private dentistry, all health care being provided for free subsidized by the government payed for by taxes. Italy has a national health service which provides approximately 75% of their care, Dental care in Sweden is free for children and subsidized for adults. In Japan dental fees are set by the government which then covers 70% of the cost with the individual expected to pay 30%. Most of the European countries subsidize all or most of dental care for children and at least some dental care for adults.
This is a highly effective strategy for the provision of health care and it is one that we have not chosen to pursue in this country. So the question that we are facing here in Yolo County, is in the absence of a comprehensive, free or heavily subsidized universal dental service, with enough dentists available to meet the currently unmet need, how can we optimize the availability of fluoride ( admitted by the opponents to be safe and effective when applied topically ) and demonstrably safe at the proposed level ? I would propose that at this point in time, with health resources distributed as they are, fluoridating the water to the 0.7ppm level is a both safe, and effective strategy.
If all these well-meaning Davis professionals want to drug my family’s water, they had better put it to a citywide vote.
Terri Leonard’s data seemed very convincing to me as I read it and pondered the World Health Organization data. Here we have similar trends resulting from fluoridated water use and fluoridated salt use and no use of fluoride? And, there’s the most dramatic drop in Iceland, one of the “non-fluoridated countries.”
This pretty well debunks the idea that fluoride is what is causing the declines in tooth decay, right?
Then, it turns out that medwoman got up early today and fills in the critically missing piece of information. “Non-fluoridated countries” is a misnomer. How many of those countries with impressive reduction rates actually are “high fluorided countries” in that citizens have nearly universal topical application (and, of course, have no need for water or salt options).
How could the World Health Organization release such a misleading graphic as the first one regarding “non-fluoridated countries” with only a tiny footnote (that I’d missed on first reading) that redefines what the meaning of “non-fluoridated country” could be. Maybe these really aren’t WHO charts after all.
It may be that Terri Leonard wasn’t aware of the fatal flaw in the evidence she offered here. But, it makes obvious how difficult it is for we scientifically challenged folks to evaluate arguments and to make educated votes. If such an impressive presentation is so misleading as to almost qualify as a lie, what about the letters of the editor that are little more than slogans built on such articles?
Medwoman stated that water fluoridation is “demonstrably safe at the proposed level.” On the basis of what controlled safety studies?
Medwoman stated “Topical application is another effective option, but implies ready and affordable access to a dentist who can apply fluoride topically, and or a pediatrician who can prescribe drops.” Topical fluoride includes toothpaste, and we could buy a lot of toothpaste and toothbrushes with the money it would take to fluoridate our water. Also, drops are swallowed, not used topically.
The reason that we are seeing a decline in tooth decay in all industrialized countries is the propensity of fluoride in toothpaste and mouthwash, the affordability of toothpaste and toothbrushes as a result of free market capitalism and global competition and the success of health education in the industrialized world.
Put fluoride in the water of all third-world countries.
Don’t put anything in the water of industrialized countries… except for what is required ONLY to keep the water safe and clean.
The absurdity of this continued practice is only exceeded by the absurdity of those in the medical profession that continue to push it. The road to being over-medicated is paved with the good intentions of the medical profession. If doctors want to over-medicate me and my family, at least give me the option to resist.
When (as a WAC member) I received Dr. Leonard’s e-mail on Saturday I responded to her (with copies to the WAC Chair and Dianna Jensen) as follows:
[i]”Terri, for Brown Act reasons I do not respond to you with Reply All, but I ask Dianna Jensen and Elaine Roberts-Musser to include this e-mail and your response as part of the official WAC materials and share them at the appropriate time with all the WAC members.
With that said, you present the material below as if the decision on fluoridation is an “either/or” decision. Why is that? Said another way, what prevents fluoridation from being a “both/and” decision?
Thank you for your consideration of this question.
Sincerely,
Matt Williams “[/i]
Thus far I have received no response from Dr. Leonard. Hopefully she will respond here so everyone can have the benefit of her response. When one looks at the significantly increased presence of processed sugars in the diet of most Americans, it certainly appears that we need all the tooth decay fighting tools we can possibly have. I hear loud and clear the concerns about high levels of fluoridation, but we aren’t talking about proposed levels that come anywhere near those high levels. Barbara King is correct when she says “Topical fluoride includes toothpaste, and we could buy a lot of toothpaste and toothbrushes with the money it would take to fluoridate our water” but buying them is only part of the solution. Ensuring that they are both distributed and then used is key to making them effective. The question that I keep coming back to is why can’t we be pursuing a both/and approach . . . [u]both[/u] topical modalities [u]and[/u] appropriately low levels of fluoridation [u]and[/u] improved dietary practices. We have naturally occurring fluoride in our current well water and there doesn’t appear to be any substantial (or reported) problems with hypersensitivity or fluorosis or diminished IQ or any of the other suspected concerns. So why is this issue being couched by the anti-fluoride proponents in either/or terms?
Frankly
[i]”If doctors want to over-medicate me and my family, at least give me the option to resist.”[/i]
Frankly, you have the option to resist. Resistance is not futile. All you need to do is go to the distilled water aisle in your grocery store, or install a filter underneath your sink.
Just as Mr. Byrns could have saved his two beloved english cars if he had invested in a sprinkler system for his garage, you have the option to go to the distilled water aisle in your grocery store, or install a filter underneath your sink.
Matt,
That is not acceptable. I have one plumbing system. It is MORE than inconvenient to purchase and lug water consistently enough to ensure that I never ingest this known toxin. How to I prevent it from getting on my food? From being ingested when I shower or wash my hands? How to I keep it from going into the soil of my garden? The “bottled water” argument is a non-starter and is very weak. If you are going to make the “choice” argument, then we would need two plumbing systems going to each property.
[quote]The graphs put forward by Dr. Leonard are not in dispute and certainly show a decrease in cavities across many populations. However, they do not refute the point made by Dr. Lyman, nor do they tell the whole story about the various reasons for the drops in dental caries across countries.
The point Dr. Lyman was making was a specific one that some countries have chosen ingestion of fluoride in mild or salt as an alternative to water, not that this was the only alternative. Topical application is another effective option, but implies ready and affordable access to a dentist who can apply fluoride topically, and or a pediatrician who can prescribe drops.
[/quote]
No, medwoman, that was not the point that Dr. Lyman was making. Anyone interested in hearing what Dr. Lyman said should visit [url]http://archive.cityofdavis.org/media/[/url] and click on Water Advisory Committee Archives for Thursday, April 25, 2013. Mark Siegler’s first question, regarding the WHO graphs, starts at 1:27:48 (1 hour 27 minutes 48 seconds), and Dr. Lyman’s response follows. One can fast forward to that part of the video. At 1:41:00 is where Mark Siegler asks for clarification regarding whether it is the position of the pro-fluoridation presenters that the low caries rates in populations that are not drinking fluoridated water is due to the consumption by those populations of other fluoridated products, such as milk. Dr. Lyman’s response follows.
In his responses to Mark Siegler’s questions, Dr. Lyman was not saying or implying anything at all about topical application of fluoride, and he was not saying that topical application accounts for the decrease in caries rates in countries that do not fluoridate their water. He was making a shocking and inaccurate statement that the decrease in caries rates in countries that do not fluoridate their water is due to fluoridation of their milk or salt instead.
Dr. Leonard, since you dispute the statement that “the decrease in caries rates in countries that do not fluoridate their water is due to fluoridation of their milk or salt instead,” what is the point of your letter/article?
Why did you not indicate the real reason, the use of topical fluoride in countries that have near universal dental care? Why did you present a chart that implied these countries are “non-fluoride countries”?
It appears your purpose is to discredit Dr. Lyman rather than to correct what seems to be a simple misstatement. (Would you’ve agreed with him if he’d added topical fluoridation to his incomplete list of milk and salt fluoridation?)
[quote]Why did you not indicate the real reason, the use of topical fluoride in countries that have near universal dental care? Why did you present a chart that implied these countries are “non-fluoride countries”? [/quote]
You are trying to put words in Dr. Leonard’s mouth while making a statement for which you have no evidence. The point Dr. Leonard was making is that you do not have to ingest fluoride to get decreased cavity rates and she simply pointed out that Dr. Lyman was flat out wrong when he said otherwise. Further, how do you know the “real reason” all of these countries have very low caries rates is “the use of topical fluoride in countries that have near universal dental care?” Maybe all they have is a real good program to teach their kids good dental hygiene habits including brushing, flossing, and mouthwash. Maybe they never have to go to the dentist at all to get fluoridated lacquers. Please do your research before making broad, unsubstantiated assertions.
Dr. Leonard was absolutely correct that Dr. Lyman was trying to give the incorrect information that you need to ingest fluoride to make it work. Whether he mispoke or not, Dr. Lyman knew, or should have known, that his statement was factually untrue and not supported by any evidence. He appeared to me to try to make up evidence on the spot to validate his untrue statement and put his foot in it as a result. Don’t disparage Dr. Leonard for pointing out an obvious error which would have otherwise lent credibility to the assertion that fluoride has to be ingested to work and everybody in Europe does it. That is not true. Many do not ingest fluoride in Europe, via drinking water or otherwise in salt or milk, and their caries rates are as low or lower than in the US. Come to the WAC meeting this Thursday and you will see substantial additional empirical information that drinking fluoridated water does not prevent caries.
Frankly said . . .
[i]That is not acceptable. I have one plumbing system. It is MORE than inconvenient to purchase and lug water consistently enough to ensure that I never ingest this [b]known toxin[/b]. How to I prevent it from getting on my food? From being ingested when I shower or wash my hands? How to I keep it from going into the soil of my garden? The “bottled water” argument is a non-starter and is very weak. If you are going to make the “choice” argument, then we would need two plumbing systems going to each property.”[/i]
Frankly, you do know that you are currently ingesting fluoride in your Davis water at a level that is approximately 50% of the proposed level. Are you saying that you want Davis to remove that naturally occurring level of fluoride from your water?
[i]Ingested when I shower or wash my hands? [/i] Come now. You are much smarter than that. You are beginning to sound like Michael Harrington. 8>)
[i]Frankly, you do know that you are currently ingesting fluoride in your Davis water at a level that is approximately 50% of the proposed level.[/i]
That’s right. So the city is planning to double the level of this toxin in my water. That is unacceptable.
[I]Come now. You are much smarter than that. You are beginning to sound like Michael Harrington[/I]
I wish I was as smart as Mike along with my existing high levels of emotional intelligence. I would be much more effective!
I need to find the article, but yes, you will absorb a certain about of the trace elements and toxins in water by simple skin contact.
Just saying…
[quote]“Non-fluoridated countries” is a misnomer. How many of those countries with impressive reduction rates actually are “high fluorided countries” in that citizens have nearly universal topical application (and, of course, have no need for water or salt options).
How could the World Health Organization release such a misleading graphic as the first one regarding “non-fluoridated countries” with only a tiny footnote (that I’d missed on first reading) that redefines what the meaning of “non-fluoridated country” could be. Maybe these really aren’t WHO charts after all.
It may be that Terri Leonard wasn’t aware of the fatal flaw in the evidence she offered here. But, it makes obvious how difficult it is for we scientifically challenged folks to evaluate arguments and to make educated votes. If such an impressive presentation is so misleading as to almost qualify as a lie, what about the letters of the editor that are little more than slogans built on such articles? [/quote]
When you say that there is a fatal flaw in the evidence offered, and that my “presentation is so misleading as to almost qualify as a lie…” it would appear that you are not understanding the data.
The graphs and tables are convincing evidence that systemic (ingested) fluorides, such as fluoride added to water or salt, are not the reason for the decrease in dental caries rates in industrialized nations because nations that do not add fluoride to their water or salt are experiencing the same decrease in dental caries rates as nations that do. The graphs and table beg the question as to what indeed is the real reason for the decrease in dental caries rates in industrialized nations, since this decrease is [b]clearly[/b] not due to ingested fluoride. There may be multiple reasons for this decrease in caries rates, one of which could possibly be [i]topical[/i] fluoride.
You wrote [quote]How many of those countries with impressive reduction rates actually are “high fluorided countries” in that citizens have nearly universal topical application (and, of course, have no need for water or salt options).
[/quote]
Indeed. Are the low caries rates in industrialized nations due to topical application of fluoride? That may be part of the reason.
I would disagree with the implication you make in this sentence that there is no need for water or salt options [i]as long as[/i] citizens of a country have nearly universal topical application of fluoride. This also appears to be medwoman’s stance. It would appear that your and medwoman’s argument is that we should provide fluoride in the water supply because not everyone has access to topical fluoride. The data do not support this contention. On the contrary, the data in the graphs and table indicate that water and salt fluoridation are not the reason for declining dental caries rates.
Every nation in the graphs and table has access to fluoridated toothpaste. Is that the reason for the universal decline in dental caries rates in these nations? Maybe so.
Matt: “[i]Frankly, you do know that you are currently ingesting fluoride in your Davis water at a level that is approximately 50% of the proposed level. Are you saying that you want Davis to remove that naturally occurring level of fluoride from your water?[/i]”
There is scant evidence to suggest that naturally occurring fluoride in the water is in any way harmful, so why would anyone suggest spending the money to [b]remove[/b] it from the water system? Similarly, there is scant evidence to suggest that it is in any way beneficial when supplemented at 2x the concentration so why would anyone suggest spending the money to [b]add[/b] it?
The real question that should be answered…
What percentage (or even actual number since the value is likely to be very small) of the people expected to consume Davis water lack access to fluoridated toothpaste and regular dental care? I expect that percentage to be a very small number. If you take the cost of adding fluoride to the water system and divide it by the number of people who lack access to topical fluoride through other means you will likely find that you are looking at a very high cost per person that is expected to benefit from the program.
Why would anyone suggest spending our limited resources in a manner such as this that provides so little benefit for the cost?
[quote]” It would appear that your and medwoman’s argument is that we should provide fluoride in the water supply because not everyone has access to topical fluoride. The data do not support this contention. On the contrary, the data in the graphs and table indicate that water and salt fluoridation are not the reason for declining dental caries rates.”[/quote]I’m not trying to advance the pro-water-fluoride case, just trying to figure out why you wrote this. So, the graphs deal with water and salt only, but the implication is that some unknown out there is causing the “non-fluoridated countries” downward trend.
This seems very misleading to me when it’s obvious that fluoride is involved in all or most of the countries you’ve cited. medwoman says at least some of the missing link is topical application via great country dental programs. You wonder if it might be toothpaste.
Okay, but who cares if Dr. Lyman said salt or milk also might be involved?
Further Matt…since we are building a conjunctive use water system, residents will already be receiving fluoride in the water at least for a portion of the year. What is the incremental benefit expected from fluoridation of the river water?
High cost and little or no benefit. Sounds like a perfect solution.
“Just as Mr. Byrns could have saved his two beloved english cars if he had invested in a sprinkler system for his garage, you have the option to go to the distilled water aisle in your grocery store, or install a filter underneath your sink.”
It is simply not this easy. In order to avoid fluoride, one would have to install a reverse osmosis system for the entire residence not just under the sink in the kitchen. Besides being absorbed orally, fluoride is readily absorbed transdermally when showering or bathing. RO systems are very expensive and not without their own problems. One problem is that they remove ALL minerals, including the natural ones which are beneficial. One would also have to avoid eating food or drinking beverages prepared with fluoridated municipal water as in local restaurants.
[quote]One would also have to avoid eating food or drinking beverages prepared with fluoridated municipal water as in local restaurants.[/quote]
Which one would also presumably have to do in the dozens of other cities in California that fluoridate their water, including nearly every one that is within driving distance:
[url]http://davismerchants.org/vanguard/fluoridationcitiesCA.pdf[/url]
That is assuming you believe that that level of fluoride is toxic.
[quote]
Which one would also presumably have to do in the dozens of other cities in California that fluoridate their water…[/quote]
that is correct
Dr. Leonard (or anyone familiar with the data presented in the charts), would you please point me to the location of the raw data used to create the charts on Fluoride Alert’s website. I have looked for the charts and/or the raw data at the WHO referenced site and could not find it. Thanks.
tleonard
[quote]I would disagree with the implication you make in this sentence that there is no need for water or salt options as long as citizens of a country have nearly universal topical application of fluoride. This also appears to be medwoman’s stance. It would appear that your and medwoman’s argument is that we should provide fluoride in the water supply because not everyone has access to topical fluoride.[/quote]
This is not my stance. A more accurate view of my position would be that we should provide fluoride in the water supply as part of a comprehensive strategy to optimize dental care for all of our citizens given the limitations of our current health care system. I would also recommend that all of our children ( and indeed all people ) be provided with universal access to government provided dental and health care. Many of the opponents of fluoridation seem to want to use the European example as a benchmark for what we should do. Perhaps we should. Perhaps using a single party payer system such as the most of the European countries do would lead to improved dental and overall health care for our entire population as Iceland has chosen. I simply do not see this as a politically viable option in this country at this point in time. I also do not believe that Communicare has the resources to provide the care needed for the underserved at this point in time based on conversations with Communicare providers.
I am new to this argument and so am still trying to sort the facts out. The pros to fluoride seem to be that they reduce rates of dental caries. However this has only been shown to be the case when administered topically – and is the argued reason for decreased rates in non-fluoridating water countries. So I guess my question is, why advocate for fluoridating water here if its benefits are realized when ingested? If my toothpaste says “don’t swallow more than a pea-sized amount” what does drinking it in the water do for me? Isn’t fluoride kind of nasty stuff? Why not advocate for topical applications and keep it out of the water? On an aside, I grew up with fluoride in my water and had plenty of cavities. While anecdotal, I still question the ingestion of something that is known to be a toxin because it “may” benefit me when instead I can get a topical application without the potential toxic side effects (ie thyroid issues and the like).
I need to add a clarification:
“So I guess my question is, why advocate for fluoridating water here if its benefits are *not* realized when ingested?”
newbie
All good questions. Here is my short form summary of the differences of opinion.
1) There is not agreement that “it is only been shown to be effective when administered topically”. There are
many dentists who believe that there is ample evidence of benefit from ingested fluoride which then enters
the saliva providing a continuous ” topical application” since the saliva is in constant contact with the teeth.
2) The issue about not swallowing one’s toothpaste is a matter of dosage. Fluoride in toothpaste can run
as high as 5000 ppm. It is not a good idea to swallow at this level. The amount of fluoride
recommended for our water supply is 0.7ppm. To illustrate how something can be good for us at very small
amounts and very dangerous at higher levels, think of Tylenol. Two tablets are good for a headache, two
hundred will likely lead to death from liver failure. The amount is crucial.
3) No one would advocate putting ” a toxin” in the water if they did not believe that the benefits out weighed the
admittedly “potential” risks. What the proponents believe is that there is evidence of effectiveness,
and that of all the proposed toxicities, only fluorosis has been demonstrated. The others are all conjecture
with no medical evidence to support them at the proposed level in our water even after 60 years of use.
4) While anecdotal evidence is just that, a personal story, it is none the less powerful for the individual. So I
would ask you the following questions. Did you, or any one else you know get osteosarcoma related to
drinking the fluoride in your neighborhood water ? Do thyroid problems ( or any other problem except
fluorosis) occur with greater frequency in fluoridated communities than in appropriately controlled
un fluoridated communities ?
Since the current onset of this issue, I have been searching the literature for evidence of such harm from
fluoride at the proposed level and have found none. As a Women’s Health specialist, I came to this issue
neutral not having examined the issues. I have arrived at the conclusion that given the current structure of
our health care system, where not everyone has the ready access to a dentist that you and I enjoy, the most
cost effective means to provide optimal levels of fluoride for those who would most benefit is in the water
supply.
RD: The link to the WHO data is in the chart graphics. Anyone can use the link to go to Malmo University’s Oral Database online, which is part of their work as a “WHO Collaborating Center for Education, Training and Research in Oral Health.” A couple of clicks gets you to country-by-country oral health data expressed in DMFT’s (Decayed Missing and Filled Teeth.)
Frankly said . . .
[i]”That’s right. So the city is planning to double the level of this toxin in my water. That is unacceptable.”[/i]
Mark West said . . .
[i]”There is scant evidence to suggest that naturally occurring fluoride in the water is in any way harmful, so why would anyone suggest spending the money to remove it from the water system? Similarly, there is scant evidence to suggest that it is in any way beneficial when supplemented at 2x the concentration so why would anyone suggest spending the money to add it?
Further Matt…since we are building a conjunctive use water system, residents will already be receiving fluoride in the water at least for a portion of the year. What is the incremental benefit expected from fluoridation of the river water?
High cost and little or no benefit. Sounds like a perfect solution.”[/i]
The two comments above cause me to wonder whether we need a little Judgment of Solomon with respect to fluoridation in Davis.
If Solomon were able to give his judgment it might go as follows:
1) Only fluoridate the surface water, and
2) Only fluoridate the surface water up to the current naturally occurring levels of Davis well water.
When asked why he supports that solution Solomon would reply
A) Davis’ caries rate is only 16%, much lower than most communities. That means the current protocols are indeed working for all the people other than the very low-income segment.
B) As Mark West has pointed out, “There is scant evidence to suggest that naturally occurring fluoride in the water is in any way harmful.” Said another way, we are seeing no hypersensitivity to fluoride issues in Davis at the current levels.
C) Not having to add supplemental fluoride to the six deep aquifer wells will reduce the capital cost, the operating cost and the maintenance complexity. One seventh the cost makes Mark West’s statement, “High cost and little or no benefit” somewhat suspect. It certainly pulls the rug out from under the “high cost” part.
D) A conjunctive use system that introduces surface water with its low fluoride levels as the primary water supply for indoor use, will result in a reduction of the fluoride levels that appear to have been working well for Davis. Bringing the treated surface water up to the same level as the current well water eliminates the concern that frankly has raised when he says, “… double the level of this toxin in my water. That is unacceptable.”
What Solomon wants to know is whether “splitting the baby” is indeed the wisest solution given the historical data here in Davis.
ebowler said
[i]”It is simply not this easy. In order to avoid fluoride, one would have to install a reverse osmosis system for the entire residence not just under the sink in the kitchen. [b]Besides being absorbed orally, fluoride is readily absorbed transdermally when showering or bathing.[/b] RO systems are very expensive and not without their own problems. One problem is that they remove ALL minerals, including the natural ones which are beneficial. One would also have to avoid eating food or drinking beverages prepared with fluoridated municipal water as in local restaurants.”[/i]
ebowler, lets look at your bolded statement for a moment. If transdermal absorption is in fact scientifically proven, then lets do some simple exposure calculations. When you take a shower what proportion of the shower water actually comes into contact with your skin and resides there long enough to activate any transdermal absorption? I’m going to WAG a guess and say that it is significantly less than 1% of the water volume. So just exactly how much absorbed fluoride is possible in a daily shower. My WAG suspicion is that it is significantly less than the amount of fluoride you get when you ingest a glass of water.
With the above said, what I am hearing you saying is that you see fluoride in the same light as you see concentrated sulfuric acid . . . toxic at any level of exposure. Is that correct?
[b]Tooth and Nail: Fluoride Fight Cracks Portland’s Left
Liberal City Chews Over Water Vote; Debate Brings Out Mimes, Indie Rockers[/b]
[url]http://online.wsj.com/article/SB10001424127887323398204578488290293116774.html?KEYWORDS=portland+fluoride[/url]
[quote]PORTLAND, Ore.—In the 1950s, after health authorities began fluoridating U.S. water supplies, they faced opposition from groups like the John Birch Society, which called it “an unconstitutional mass medication of the public.”
Sixty years later, the fight over fluoridation has erupted in Portland, where the battle has drawn in the city’s craft-beer brewers, organic-food purveyors and environmentalists. Even some of the city’s famed indie-rock musicians are taking sides.
The debate has prompted something of an existential crisis in this self-consciously liberal city, which votes Tuesday on whether to overturn the city council’s 2012 decision to fluoridate. Citizens who pride themselves on tolerance are divided on the appropriately progressive response to fluoridated water: Is it an intrusion into personal liberty, or a compassionate public health measure? [/quote]
[quote]When you take a shower what proportion of the shower water actually comes into contact with your skin and resides there long enough to activate any transdermal absorption?[/quote]
Actually, showering is thought to provide even more exposure than bathing due to the inhalation of water vapor in addition to the transdermal effect. Transdermal absorption of fluoride is well-known, in fact, one drug company has even patented a transdermal fluoride patch for the prevention and treatment of bone loss.
Interesting, lets drill down into both those points. 1) If you collected all that water vapor that goes into the body from the the typical shower, how full would it make a water glass? 2) What is the duration of the skin contact of the transdermal fluoride patch? 3) How does that duration compare to the duration of contact of shower water in a typical shower?
Finally, are you telling me that transdermal exposure to a “toxic” substance prevents and treats bone loss? As Arte Johnson would say, “Verrrrry interesting.”
The Judgment of Solomon is looking better and better all the time.
Matt,
I think Solomon would have to consider the issue of chronic exposure versus single exposures.
Traveling to a city that fluoridates and drinking their water on an occasional basis is not the same as living in that city and using that water on a daily basis. Surely wise Solomon would have made that distinction.
Next, inhaled substances enter the bloodstream through the lungs, a fast route. Inhaling water vapor has a much greater impact than drinking an equivalent volume of water vapor , just like smoking marijuana has different effects than eating it.
Ernesto, how long have you lived in Davis?
Whatever number of days/years your answer is, that is the number of days/years that you have been exposed to a Solomon’s Judgment amount of fluoride in your water. Every single day. Every single minute of every day. Chronically.
So with that said, can you name even one single Davis resident (yourself included) who exhibits any negative effects of that chronic fluoride exposure?
Your inhaled vs ingested example is interesting if only because of the substance you chose as an example. Further, it is interesting that you chose to compare a liquid vs liquid reality to a gas vs solid reality. Out of curiosity, can you come up with a liquid inhaled vs. a liquid swallowed comparison? Some questions you might want to ask as you do are 1) What is the absorption rate of a liquid that enters the digestive tract? 2) What is the absorption rate of a liquid that enters the respiratory tract during repiration? I believe you will fins that in situations other than diarrhea, the absorption rate of a liquid is close to 100%. The absorption rate of a respired liquid is certainly well below 100% because much of the vapor is exhaled at the end of each respiratory cycle.
If you are so concerned about any and all levels of fluoride in water, why haven’t you been crusading for the removal of all fluoride from our well water during the time you have lived in Davis?
It seems like you yourself are practicing the Judgment of Franklin.
Matt Williams said:
[quote]If you are so concerned about any and all levels of fluoride in water, why haven’t you been crusading for the removal of all fluoride from our well water during the time you have lived in Davis? [/quote]
The compound found in “naturally fluoridated” waters is calcium fluoride which is far less toxic than sodium fluoride, a common fluoridation agent, or hydrofluorosilicic acid, the compound now used in over 90 percent of fluoridation programs. Hydrofluorosilicic acid is a direct byproduct of the phosphate fertilizer and aluminum industries. Less than 2% of calcium fluoride is absorbed by the body with the remainder being excreted, primarily in the urine. Unlike calcium fluoride, sodium fluoride and hydrofluorosilicic acid are retained in great amounts in the body resulting in far greater toxicity. This is the reason that you do not see fluoridation opponents lobbying for the removal of natural calcium fluoride from the water.